
Colorectal, visceral pediatric surgery & pediatric urological treatments
As the only pediatric surgeon in Austria so far, I have special training (diploma) in colorectal surgery. As the deputy head of the special outpatient clinic for colorectal malformations in children and adolescents and founder of the multidisciplinary motility center at the University Clinic of the Medical University of Vienna, I gained valuable experience in the treatment and research of many rare diseases of the colon, rectum, and genital area. I continuously treat and operate on children and adolescents with intestinal motility disorders.
My scientific expertise and my extensive experience allow me to carry out “basically simple” operations in such a way that the risk of complications is reduced to a minimum. I use all of my know-how for complex operations and work in interdisciplinary teams to achieve the best possible quality of life. For me, that means commitment and empathy for children – my aim is always to give them the highest possible quality of life.

Chronical Constipation
A wide variety of causes can lead to acute mild constipation in children. For example, with a low-fiber diet, insufficient fluid intake, electrolyte disorders, endocrinological, metabolic, neurological or psychological diseases. If your child has pain during bowel movements, they will unconsciously avoid them in the future and hold back the stool. This creates a vicious circle.
Possible symptoms
Chronic constipation (constipation) is usually present in children if it lasts longer than 4 weeks and during this time at least two “ROM IV criteria” occur at least once a week. These include: two or fewer bowel movements per week, excessive retention of stool, painful or hard bowel movements, large-diameter stools (which could “clog” the toilet), large masses of stool in the rectum, faecal incontinence or stool smear at least once a week Children who are already clean.
In addition, abdominal pain, flatulence, bulging of the abdomen, decreased appetite, premature feeling of satiety, irritability, sensitivity and excitability (irritability) can occur. These will improve immediately after you have emptied a large amount of stool.
Diagnosis and treatment
A detailed medical history and physical examination should be performed in all cases. With chronic constipation, the bowel is sluggish and dilated. Education and non-pharmacological treatment with toilet training, a reward system and a diary for defecation can lead to success, depending on the diagnosis .
If necessary, initiate pharmacological treatment including evacuation, maintenance therapy, and weaning. In any case, it can take several months for it to regain its original form and function and thus for regular, normal stool behavior.
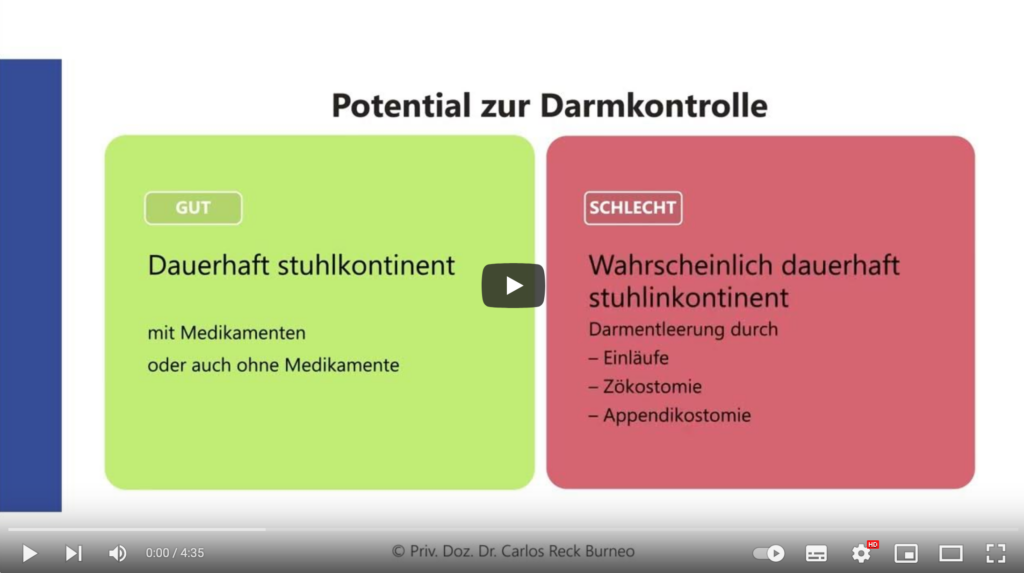
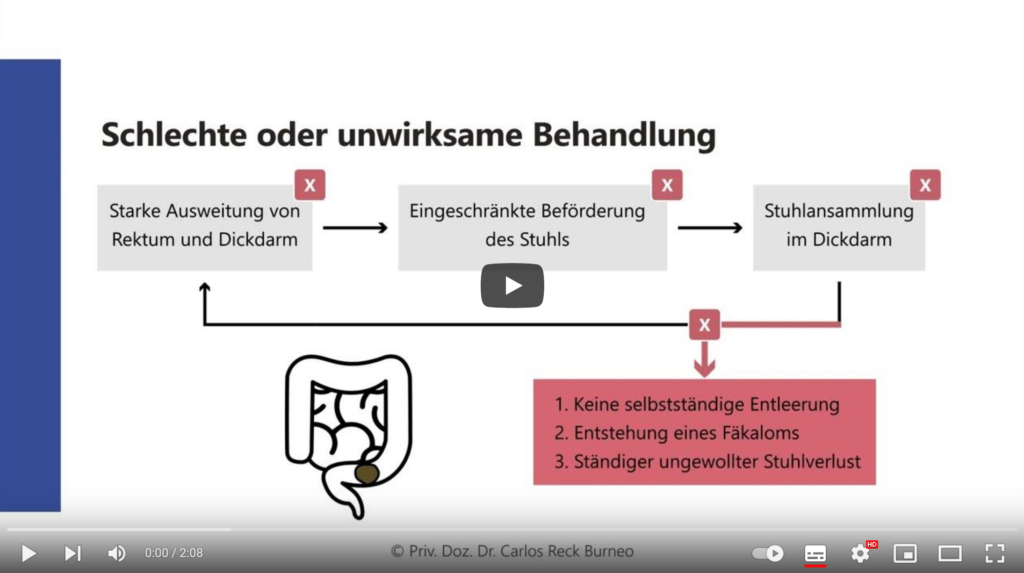
Explanatory videos: Fecal incontinence and constipation in children
These short videos are aimed at parents. It deals with fecal incontinence and constipation in children. These common problems can affect children’s quality of life and also cause psychological stress. It explains how control over bowel functions can be achieved and which treatment methods are available.
Hirschsprung’s disease
This rare malformation is congenital. In Hirschsprung’s disease, there are no nerve or ganglion cells from the anus upwards (aganglionosis). This prevents the stool from being transported further in the intestine. In many children, only the end arm (rectum or rectosigmoid) is affected. In very rare cases, aganglionosis involves the entire large intestine or even parts of the small intestine.
Possible symptoms and diagnosis
Most children are noticed relatively soon after birth because they show one or more of the following symptoms: they do not deposit meconium or they do not deposit meconium (child spitting), the stomach is very bloated, they vomit or have massive constipation that lasts up to Intestinal obstruction. A biopsy is necessary for a definitive diagnosis.
Treatment and aftercare
Hirschsprung’s disease always requires surgical treatment. During this, the affected section of the intestine is removed. Some children need a stoma, an artificial anus. After the operation, Hirschsprung’s disease patients often experience constipation or inflammation (enterocolitis). For some children, the problems subside at school age, while others also need medical support as adults. Close-knit follow-up checks or pediatric surgical follow-up care, physiotherapy, the right diet and psychological care can help.
Anorectal malformations
In children with an anorectal malformation (ARM / anal atresia) the anus / anus is completely absent or opens incorrectly.
Diagnosis and formations
If there is a fistula, it is either right next to the anatomically correct anus or it opens into the urethra or bladder. If the anus, the urethra and the vagina flow into a common canal in girls, this is known as a cloacal malformation.
A cloacal exstrophy occurs extremely rarely. It occurs in combination with an open bladder, open bowel, genital malformations, a lack of an anal opening, and a split pelvis. With all forms of anorectal malformations, further malformations, e.g. B. the heart, kidneys, spine or sexual organs.
Operative treatment
The treatment or operation of an anorectal malformation (ARM) by an experienced pediatric surgeon is essential. Based on the correct examinations, the quality of a single operation determines the further quality of life of the child. I am happy to treat your child as a specialized colorectal surgeon.
„We have had a wonderful experience with Dr. Reck-Burneo for my daughter’s care. He is extremely knowledgeable about her colorectal condition and always takes the time to answer our questions thoroughly and with excellent beside manner. We never feel rushed during appointments with him, and he is very patient with our daughter, who isn’t always calm at the doctor’s office. We have been very happy with his care and will continue to see him for follow-up appointments, even though we moved to another European country, because we have been pleased with the consistency and quality of care received.”
Shannon O.
Mother
Pediatric urology
Children and adolescents with undescended testicles or phimosis (narrowing of the foreskin) require a pediatric urological treatment.
Undescended testicle
Male fetuses develop the testicles in the abdomen during pregnancy. Shortly before birth, these migrate into the scrotum. This can lead to “getting stuck” or “wrong wandering”. Experience has shown that the position of the testicles in a newborn can still be okay in the first six months. After the sixth month of life, surgical intervention is advisable for sliding or inguinal testicles. This ideally takes place before the first year of life. Annual clinical controls are sufficient for pendulum testicles. If the testicles cannot be felt, there is unilateral or bilateral cryptorchidism, which requires laparoscopy (endoscopic examination of the abdomen).
Phimosis (narrowing of the foreskin)
Almost all male newborns have an innate “physiological” narrowing of the foreskin. This is glued to the glans and cannot yet be withdrawn. In the course of development, this bond normally loosens by itself. The foreskin is completely retractable by puberty in most cases. If this is not the case, treatment with ointments can loosen the adhesive. If this does not lead to success, circumcision should be considered.
Surgical intervention is also advisable for the following reasons: recurrent inflammation of the foreskin and glans (balanitis, balanoposthitis), chronic inflammation of the foreskin (balanitis xerotica obliterans, lichen sclerosus) or visible scarring or recurring urinary tract infections in boys. Health insurance companies do not cover circumcisions for religious reasons.
Hernias (umbilical or inguinal hernia)
An inguinal hernia in children is when the connection between the abdomen and the scrotum or labia is still open at birth. The abdominal viscera can shift into the inguinal canal, which can then lead to entrapment. An umbilical hernia is a congenital gap in the area of the belly button. Intestines or abdominal fat can bulge into these and occasionally cause discomfort. Most of the time, this gap disappears by the age of three.
diagnosis
There are bulges in the groin (inguinal hernia) or around the navel (umbilical hernia) clinically detectable. If a congenital umbilical hernia is present beyond the age of three, surgical closure of the gap is advisable (before entering school).
Operative treatment
The interventions are mostly carried out on an outpatient basis under regional anesthesia. In the case of a hernia, the open connecting channel in the groin is exposed and sewn through a tiny cut. This quickly eliminates the risk of entrapment. The operation of an umbilical hernia is also carried out painlessly on the sleeping child. The procedure consists of a tiny incision below the navel. Then the small gap in the abdominal wall is exposed and sutured.